Breathing circuits are the interface between the ventilation or anaesthesia machine and the patient's airway. They are the first line of defence against cross-contamination, the main determinant of inspired gas quality and a critical factor in the flow resistance the patient or ventilator must overcome. The wide variety of types — corrugated, accordion, extensible, with or without a water trap, with or without access ports, in different materials — confuses buyers without a clear selection guide.
Anatomy of the breathing circuit: components and functions
A dual-limb breathing circuit has several components. The inspiratory limb carries fresh gas from the ventilator or anaesthesia machine to the patient and is the pressurised limb. The expiratory limb carries expired gas back to the ventilator and holds condensation water. The Y-piece joins both limbs and connects to the endotracheal tube; it is the most-handled point and the highest risk of accidental disconnection. The water trap, at the lowest point of the expiratory limb, collects condensate to keep it from reaching the ventilator or patient. The in-line filter between the Y-piece and the endotracheal tube acts as an extra barrier. Proximal connectors follow the 22/15 mm ISO 5356-1 standard. Optional access ports allow temperature, end-tidal CO₂ or additional gas delivery. Understanding each component lets you quickly identify the cause of a ventilation alarm.
Standard corrugated circuit: the most used in ICU and anaesthesia
The corrugated circuit is the most produced and used type in the world. Its spirally ribbed walls give flexibility and compression resistance, letting it bend without collapsing the lumen. Internal diameter is 22 mm for adults and 15 mm for paediatric/neonate, per ISO 5367 for universal compatibility with ventilators, anaesthesia machines and accessories from any manufacturer. Most PVC circuits are transparent, letting you see accumulated condensate and detect secretions or blood.
Guidelines recommend changing every 7 days in anaesthesia (a new circuit per surgical patient for use over 3 hours) and every 48–72 hours in continuous mechanical ventilation, unless visibly contaminated sooner. The limitation of the standard corrugated circuit in paediatrics is its greater dead space at 22 mm diameter, which can matter in patients with very small tidal volumes.
Accordion extensible circuit: for maximum flexibility

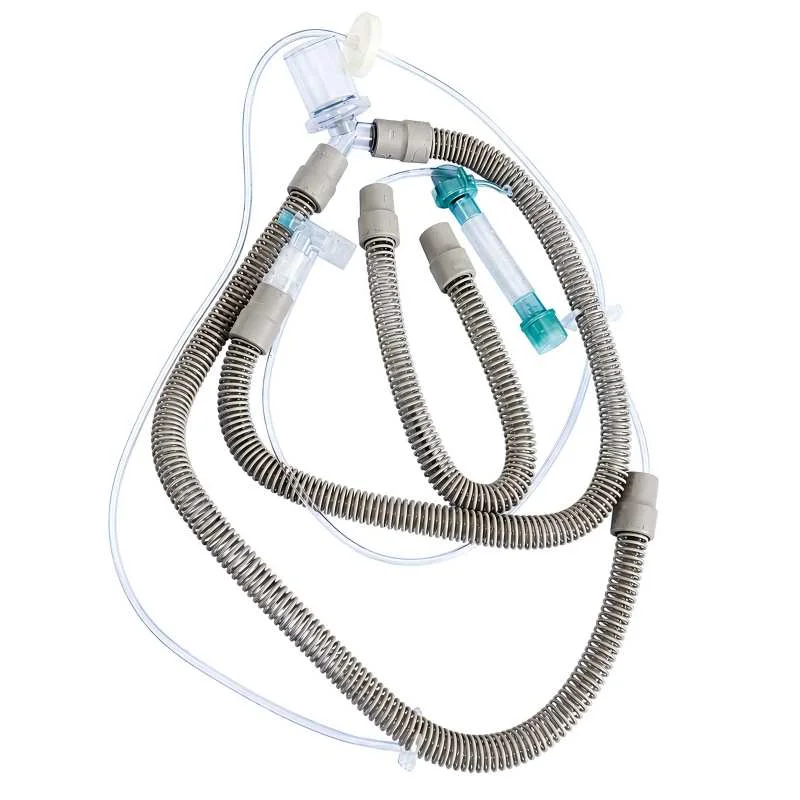
The accordion extensible circuit is designed where maximum flexibility is needed without kinking risk, able to lengthen or shorten with patient position. Its concentric multi-chamber structure compresses the circuit to a third of its working length when not in use. It is preferable to the standard corrugated circuit in head and neck surgery, where the surgical field occupies the space the circuit would normally use, and in procedures with frequent position changes such as prone spine surgery. In critical transport, the ability to compress the circuit eases storage and handling on stretchers with limited space. It combines extensibility with the corrugated structure and its integrated water trap can sit at any point along the circuit.
Circuit with multifunction filter extension
The circuit with a multifunction filter extension combines, in a single component, the extension tube, an HME filter and access ports for temperature, capnography and nebulisation. This integrated design reduces the number of pieces, lowers potential disconnection points and simplifies assembly. It is the preferred solution in modern ICUs where circuit standardisation is a priority to reduce assembly errors.
The integrated filter has >99.9% bacterial and viral efficiency with a 40–45 mL dead space suitable for adults. The lateral nebulisation port allows bronchodilator nebulisation without removing the filter, using a vibrating-mesh nebuliser compatible with a closed circuit. The trade-off: if the filter saturates prematurely with abundant secretions, the whole unit must be changed. For high-secretion patients, a separate replaceable HME/HMEF filter may be more economical.
Standard ICU ventilator circuit

The standard ventilator circuit is the routine choice in ICU for prolonged invasive mechanical ventilation. It is designed to minimise condensation and to be compatible with the most widespread ventilators: Dräger, Hamilton, Maquet Servo, GE Carescape and others.
Features include: high-capacity water traps on both limbs to reduce emptying frequency; an inner tube with a hydrophobic surface that reduces condensate adhesion; twist-lock connectors to prevent accidental disconnection; a temperature port on the Y-connector for direct expiratory temperature probe connection; and compatibility with an active humidifier by connecting the humidification chamber on the inspiratory limb. The choice between an HME filter or active humidifier with this circuit depends on ventilation duration, secretion volume and patient temperature.
The manual resuscitator (BVM): emergency ventilation
The bag-valve-mask resuscitator (BVM) is the most important manual ventilation device in emergency medicine. It is part of every crash cart, prehospital emergency bag and OR emergency kit. It consists of the self-inflating bag, the one-way valve that prevents rebreathing of expired gas, and the mask or endotracheal tube adapter.
The adult BVM has a 1,600 mL bag, though the delivered tidal volume is 500–600 mL per one-handed squeeze. AHA 2020 CPR guidelines recommend 500–600 mL (6–8 mL/kg ideal weight) for adults, so one-handed compression is generally enough and reduces hyperinflation risk. The oxygen reservoir connected to the intake valve raises FiO₂ to 85–100% with O₂ at 10–15 L/min. Without the reservoir, the maximum FiO₂ does not exceed 40–50% even at high flow.
Anaesthesia circuit filter kit
In anaesthesia, the breathing circuit is shared during the procedure between vaporised anaesthetic, O₂ and the patient's expired CO₂. Microbiological contamination of the anaesthesia circuit is a real concern: Pseudomonas aeruginosa and Staphylococcus aureus have been isolated in unfiltered anaesthesia machine tubing.
The filter kit integrates a high-efficiency HME filter (>99.97% MPPS) at the interface between the circuit and the endotracheal tube or laryngeal mask. This filter acts as a barrier between the patient and the machine circuit, allowing the same circuit to be used for multiple patients with the filter replaced between patients, per anaesthesia guidelines in resource-limited settings. The kit includes the HME filter, a flexible 90° elbow to orient the circuit and an adapter for LMA type I–IV laryngeal masks. The flexible connection works much like the catheter mount.
Connector compatibility: why the standard matters
Discovering that the circuit isn't compatible with the service's ventilator or anaesthesia machine is one of the most frustrating problems in clinical practice. Connectors follow ISO 5356-1, which sets standard diameters for anaesthesia and ventilation connections. The two critical dimensions are the 22 mm male connector for the circuit-patient connection and the 15 mm female connector for the endotracheal tube connection.
A non-ISO-certified circuit may have ±0.5 mm tolerances that create loose, leaking connections. The Y-piece has a 22 mm female connector toward the circuit and a 15 mm male connector toward the endotracheal tube; never try to connect the corrugated tube directly to the endotracheal tube without the correct Y-piece. When buying circuits from a new supplier, always physically test the connection with the service's equipment before a large order, and ask the supplier to explicitly state the ISO standard met.
We manufacture corrugated, accordion-extensible and BVM circuits with connectors calibrated to ISO 5356-1, CE / ISO 13485 and full lot traceability. Tell us which ventilators your unit uses and your estimated monthly volume, and we'll send you a quote on WhatsApp.
Frequently Asked Questions
How often should the breathing circuit be changed in ICU?
Current guidelines recommend changing every 7 days for mechanical ventilation circuits. More frequent changes don't reduce VAP rates but increase cost and the risk of accidental disconnection during the change. Change sooner if the circuit is visibly contaminated, has detected leaks or the HME filter is saturated.
Can I use the same circuit for high-PEEP ventilation?
Standard corrugated PVC circuits withstand working pressures up to 40–60 cmH₂O, covering most conventional mechanical ventilation including PEEP of 15–20 cmH₂O. For high-frequency oscillatory ventilation or other extreme-pressure modes, circuits specifically designed for that mode are required.
Must the breathing circuit be changed between each surgical patient?
The standard recommendation is a circuit change per patient in major surgery over 3 hours or in patients with active infection. For short surgeries in non-infected patients, many services use a high-efficiency HME filter at the patient-circuit interface and reuse the circuit for multiple same-day patients, replacing only the filter — a practice accepted by European Society of Anaesthesiology guidelines in resource-limited settings.