A negative-pressure drain (Jackson-Pratt or Hemovac type) actively evacuates the blood and fluid that build up after surgery, helping the wound heal and preventing seromas and haematomas. The carer and the patient discharged with a drain always have the same questions: "how do I empty it?", "how do I keep the suction?", "how much and how is it measured?" and "when is it removed?". This guide sums up the step-by-step handling, output recording and warning signs, plus what to check when buying drains wholesale for theatre, ICU and distributors.
How it works and why the vacuum matters
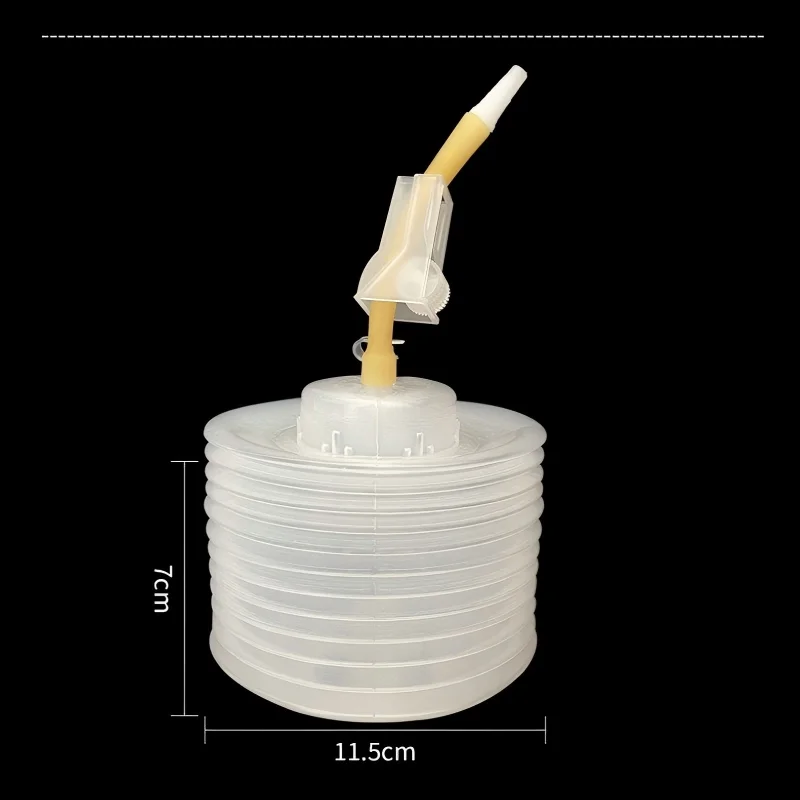
A negative-pressure drain is an elastic reservoir (bulb or bellows) connected by a tube to the operated area. By compressing the reservoir and closing it, a gentle continuous suction is created that draws fluid into the bulb. The vacuum does the work: if the reservoir is expanded (full of air or fluid), it stops suctioning and fluid builds up in the tissue.
Two common types:
- Jackson-Pratt (JP): a "grenade" or pear-shaped, low-volume reservoir; general, breast and plastic surgery.
- Hemovac: a larger-volume bellows reservoir; surgeries with more output (orthopaedics, abdominal).
Keeping the system closed and under vacuum is the key to its effectiveness.
How to empty the drain and restore the vacuum
The reservoir is emptied when it is half to two-thirds full, or at least every 8–12 h (per instruction). Procedure:
- Hand hygiene and gloves.
- Open the plug of the reservoir without touching the inner part.
- Empty the contents into a graduated container, without touching the spout against the container.
- Restore the vacuum: with the plug still open, fully compress the reservoir (squeeze the bulb or collapse the bellows) and, keeping it compressed, close the plug. On release, the reservoir should stay collapsed: that confirms there is vacuum. To create the vacuum properly, squeeze the bulb until your fingers feel the palm of your hand before closing the plug. As a routine, empty the drain twice a day (morning and evening) or when it is half full.
- Clean the spout with antiseptic before closing.
- Secure the drain to clothing with a safety pin or holder, without tensioning the tube or letting it hang below the reservoir.
If the reservoir re-expands after closing, there is a leak (plug not closed or a loose connection): check it, because without vacuum it does not drain.
Measure and record the output
Recording the output (amount and appearance of fluid) guides the decision to remove the drain:
- Measure the volume in the graduated container at each emptying and note the time.
- Record the appearance: sanguineous (blood), serosanguineous (pink), serous (pale yellow) or purulent.
- Keep a 24 h total: the trend matters more than a single figure.
Tube "milking": if there are clots, the tube can be milked by sliding the fingers from the wound toward the reservoir to keep it patent, per the surgeon's instruction.
The drain is usually removed when output falls below a threshold (often <30–50 ml in 24 h, depending on the procedure and the surgeon's judgement) and the fluid is serous. Removal is performed by healthcare staff.
Warning signs
Contact the surgical team or go to the ER if there is:
- A sudden increase in output or abundant fresh red blood.
- The reservoir does not hold the vacuum despite re-setting it (persistent leak).
- Fever, redness, warmth or growing pain around the exit site, or pus draining.
- A bad smell from the drained fluid.
- The tube comes out partly or fully, or it blocks and stops draining while the area swells.
- Severe pain when emptying or moving the drain.
Keep the insertion point clean and dry, with a dressing per instruction, and do not submerge it (showering yes, per the surgeon; bath immersion no).
How to choose negative-pressure drains
For theatre, ICU or distribution, the first call is the reservoir type and volume: the low-volume Jackson-Pratt or the larger-capacity Hemovac, depending on the surgery; what's critical is that the reservoir holds the vacuum reliably, which is exactly where they fail most. A visible graduation to measure output without transferring helps a lot, along with an anti-reflux plug that closes securely. The drain tube should have a multi-perforated atraumatic tip, length markings and a connector that won't come loose. All sterile (EO), individually packed, latex-free and with ISO 10993 biocompatibility.
We make negative-pressure drains with a graduated reservoir and reliable vacuum, in different volumes, with CE / ISO 13485 and lot traceability for tenders; ask us for samples and, if you need it, we make them under your brand. We'll sort it out on WhatsApp.
Frequently Asked Questions
How do you empty a Jackson-Pratt drain?
With clean hands and gloves, open the plug, empty the contents into a graduated container, then — with the plug still open — fully compress the reservoir and, keeping it compressed, close the plug. On release, the reservoir should stay collapsed: that confirms the vacuum has been restored.
How do I know the drain has vacuum?
After closing it while compressed, the reservoir should stay collapsed or flattened. If it re-expands or fills with air, there is a leak (plug not closed or a loose connection) and the drain is not suctioning; it must be checked, because without vacuum fluid builds up in the tissue.
When is the drain removed?
It is usually removed when the 24-hour output falls below a threshold — often less than 30 to 50 ml, depending on the procedure — and the fluid is serous (pale yellow). The decision and removal are performed by healthcare staff per the surgeon's judgement.
How often is the drain emptied and measured?
It is emptied when the reservoir is half to two-thirds full, or at least every 8 to 12 hours. At each emptying the volume is measured in a graduated container and the time and appearance (sanguineous, serosanguineous, serous or purulent) are recorded, keeping a 24-hour total.